



The Final Report - Yeti Airlines 691
An analysis based on my preliminary report and the investigation's conclusions
Visit the Evidence Files Facebook; Like, Follow, Subscribe or Share!
Find more about me on Instagram, Facebook, LinkedIn, or Mastodon. Or visit my EALS Global Foundation’s webpage page here.
In February of 2023, I wrote about the Yeti Airlines Flight 691 crash in Nepal, which occurred about a month prior to my post, utilizing publicly available information and the content of the preliminary incident report. Nepal’s Aircraft Accident Investigation Commission (hereafter, “AAIC”) recently released its final report in consort with the Civil Aviation Authority of Nepal (CAAN). This article examines that final report in juxtaposition to my initial analysis.
Note that an investigation of any airline crash is not to focus upon where to lay blame. Rather, the goal is to uncover deficiencies to correct them in order to prevent future incidents, making air travel safer for everyone. Instead of restating the totality of the facts as known at the time, this article only addresses the specifics in the final report relevant to causation. For the full recitation of the events leading up to the crash, please click on the link below.
**Note that page numbers in parentheses below indicate the page number where the content lies in the final report.

A brief summary of the facts related to the flight are necessary to position the reader for the following examination. Yeti Airlines Flight 691 (YT691) crashed in Pokhara, Nepal on January 15, 2023. Operating the flight was aircraft 9N-ANC, an ATR-72-212A/500. The ATR-72 is a twin-engine turboprop plane manufactured by Avions de Transport Régional (Italian: Aerei da Trasporto Regionale), a joint venture company of Airbus and Leonardo. A short hauler, the ATR-72 seats up to 72 people, has a range of about 852 miles (1,370 km) and flies to a maximum height of 25,000 feet fully loaded. This flight included 68 passengers and 4 crew.
The weather at the time was calm and sunny. Pokhara International Airport (VNPR) had opened just 14 days earlier, on January 1. Because VNPR’s instrument landing system (ILS) was not yet operational, YT691 was conducted under visual flight rules (VFR). This means that pilots must be able to see to certain distances, including making visual contact with the runway, in order to safely operate and land the flight.
The plane travelled from Kathmandu Tribhuvan International Airport to Pokhara with no issues. Upon its approach to VNPR, air traffic control (ATC) assigned the flight to runway 30. Airport runways are numbered by the cardinal direction they face. Thus, a runway numbered “30” indicates that it extends in an orientation of 300◦ on a radial compass (roughly west-northwest). ATC typically selects the landing runway based on atmospheric conditions and other factors, such as traffic.
Wind in Pokhara that day was minimal, 3 to 5 knots, and visibility was at about 3.7 miles (6 km). Newly opened, the airport did not have any significant traffic around the time of the incident. Nonetheless, the flight crew requested to land on runway 12 (the opposite end) instead of 30. With less than a minute remaining before expecting to land, YT691 suddenly veered into a sharp left bank from a low altitude. It struck the ground at 10:57 in a small gully along the Seti-Gandaki River, killing everyone on board.

My Initial Focus Related to Causation
My conclusion from an analysis of the evidence made available with the preliminary report led me to the following statements:
Based on the report, video of the incident, and the local weather conditions, it appears that YT691 crashed primarily from an aerodynamic stall resulting from a lack of thrust in both engines. Investigators must uncover the reason for the feathering condition of both engines.
This is precisely what the final investigation concluded. ‘Feathering’ refers to a condition when propellor planes lose thrust—either due to mechanical or other failure or purposeful action by the pilot. In this state, the blades continue to turn, primarily to reduce drag and lessen the load on the other (presumably) operating engine. In this instance, both engines ended up in a feathering condition at low altitude, leaving insufficient airflow over the wings which caused an aerodynamic stall and loss of airworthiness.
The pilots seemed surprised and/or confused by the lack of power, suggesting that neither of them purposely instigated the propeller feathering. A mechanical causation thus cannot be ruled out, especially in light of at least one unexplained Master Caution alert.
Master Cautions are alerts in a cockpit that include both audio and visual cues. Master Cautions can indicate any number of issues and typically require further investigation by flight crews.
As both pilots were experienced, it seems unlikely… that the incident began with an unforced error, but it cannot yet be ruled out that one or both pilots responded to some problem in an ultimately tragic and mistaken way. It also remains possible that a mechanical failure occurred at a critical moment of the flight from which recovery was impossible no matter how the pilots responded. Hopefully, further investigation will lead to conclusive findings. Since their introduction in 1989, ATR-72s have been involved in just 66 accident events globally, with only 12 of those involving fatalities. YT691 has the unfortunate distinction of being the first ATR-fatality incident in Nepal.
Maintenance
At the time of the release of my post, maintenance records for 9N-ANC were unavailable. I considered the possibility of mechanical issues as the primary causation, mentioning it in various places:
Mechanically speaking, it is possible that a spurious auto-feather in both engines could happen, especially if the aircraft had a bad maintenance record, but the odds remain extremely low…
The pilots seemed surprised and/or confused by the lack of power, suggesting that neither of them purposely instigated the propeller feathering. A mechanical causation thus cannot be ruled out, especially in light of at least one unexplained Master Caution alert…
It also remains possible that a mechanical failure occurred at a critical moment of the flight from which recovery was impossible no matter how the pilots responded.
[Emphasis added]
I was unwilling to summarily rule out a mechanical failure because I simply did not have enough evidence at the time to do so. Despite this, I found it exceedingly improbable that the incident occurred because of a specific mechanical failure based on the available evidence and fact pattern. This turned out to be correct. AAIC reported that all scheduled maintenance had been conducted and no planned maintenance was pending, nor did AAIC identify any problems with the aircraft before or during the accident flight [p. 22].
The Lack of Thrust
When conducting my preliminary analysis, I was particularly confounded by the apparent auto-feather and loss of thrust in both engines. Propellor engines in a feather state receive no thrust from the engines. The propellors merely spin to reduce drag from incoming airflow. A spurious auto-feather simply means that an engine reduces to a non-thrust (auto-feather) status without a mechanical cause or pilot input. In other words, it is an unexpected switch to a non-thrust condition of the engine(s) despite the engine working properly.
The idea that this could occur simultaneously in both engines of the Yeti ATR struck me as virtually impossible. In reviewing dozens of other cases involving ATR planes, I found only one instance in which a so-called “spurious” auto-feather led to a crash, and it occurred in just one of the two engines. That happened to TransAsia Airways Flight 225, which involved an ATR 72-600 that crashed in the Keelung River in Taiwan, about 3 miles from takeoff, in 2015.
Investigators learned that the events leading up to that crash started with a “spurious auto-feather” in one engine that resulted from a malfunction in the automatic takeoff power control system (ATPCS)—essentially, a software fault. The pilots of TransAsia responded to the loss of thrust by erroneously killing power to their only remaining operative engine while at an altitude no higher than 1,630 feet. They knew they lost power, but incorrectly diagnosed which engine suffered the failure.
In deference to the YT691 flight crew, I gently resisted the idea that one of the pilots could have mistakenly set one or both of the engines to auto-feather. On this, I wrote:
[I]t is also possible that one of the pilots erroneously disengaged the remaining active engine, but so far, no evidence has been provided to reach any conclusion. In fact, the report’s description of the pilots’ activity following the Master Caution suggests this was not the case.
At the time, I was adopting the possibility that one engine did spuriously switch conditions. There remained a chance that, like the TransAsia flight crew, the Yeti pilots responded by incorrectly disabling the still operative engine. That both engines entered a feathered condition required investigation; certainly, a spurious auto-feather condition shift in one engine followed by a pilot disabling the other could explain it. To explore the idea, I examined the orientation of the various flight controls and pondered whether this setup might indeed contribute to this type of pilot error.
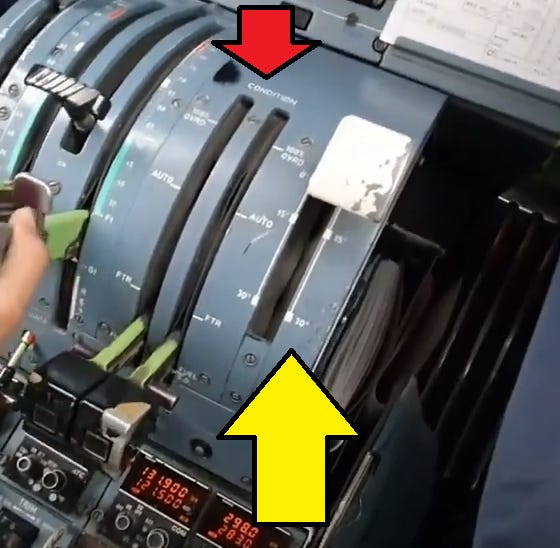
The picture above—which is not from the incident flight—is helpful to illustrate the relevant controls for flaps and [propellor condition in the ATR], which are positioned right next to each other. The yellow arrow points to the flaps controls. The upward position of the lever indicates that the flaps are not deployed. One step down extends them to 15◦ and another step down extends them to 30◦. The levers under the red arrow indicate the propeller condition. In the image, the condition levers are both in “fuel shut off” mode. The next step up is the “feather” position (FTR). During flight, the condition levers should be set to “auto,” the second-to-the-top position.
While it seems inconceivable that an experienced pilot could mistake the flaps lever with the condition levers—there are two condition levers, one for each engine—it remains curious that the shift downward from “auto” to “feather” is nearly parallel to the lever position for flaps 15 to 30. It is also worth noting that when the propellers entered a feather condition on YT691, the cockpit voice recorder (CVR) picked up a single Master Caution chime. The report does not indicate the position of the condition levers at the time of the incident, but it does note that both engines were running in “flight idle.” This happens when the propellers are feathered to prevent over-torque. The engines were in flight idle despite the power lever angle ranging between 41 and 44%.
To help contextualize this, when the propellers entered the auto-feather state on YT691, the pilots were configuring the aircraft for landing. Part of this process includes deploying the flaps at certain stages based on the speed of the aircraft. The method for moving these levers differs—the flaps lever requires a slight lift upward followed by a slide and click into the next position.
The levers that control the feathering condition of the propellors each have a trigger underneath that must be depressed to move them. Moreover, there is but one flap lever and two condition levers—one for each engine. Given the very different hand movements required to manipulate these levers, I found it nearly inconceivable that experienced pilots could mistakenly move the wrong ones. Indeed, Magnar Nordal, an ATR pilot himself, concurred in a video explainer on his YouTube channel.
Yet, the final report found the cause to be exactly that. Investigators wrote:
The most probable cause of the accident is determined to be the inadvertent movement of both condition levers to the feathered position in flight, which resulted in feathering of both propellers and subsequent loss of thrust, leading to an aerodynamic stall and collision with terrain. [pg. 68]
Remarkably, investigators concluded that the cause boiled down to one of the pilots inadvertently disabling power from both engines by moving the condition levers in place of the flaps lever. Losing power at such a low altitude ultimately led to an aerodynamic stall.
In my original piece, based partly on a video posted on YouTube showing the last seconds of the flight, I concluded with certainty that an aerodynamic stall was the final physical cause for the last erratic motion of the plane prior to impact. In the video, at just the 2-second mark, you can see two defining features illustrating it. (I won’t embed the video here to avoid opening any emotional wounds, but it is linked above).
The video shows the nose of the aircraft in a slightly pitch-up attitude, suggesting a slow speed, which makes sense for a plane on approach. As the aircraft turns toward the airport, the left wing dips precipitously, exhibiting a drastic loss of lift. With both engines producing no thrust, the aircraft was already facing diminishing lift. Activating the ailerons by turning the yoke to conduct a turn further reduces lift on the relevant wing by disrupting the airflow around it. Having very little air supporting the wings already, the disruption caused by the aileron movement instigated a sudden complete loss of lift under that wing, thereby jolting the aircraft into a severe bank in the direction of the turn. This occurred at just under 400 feet, a height from which recovery was impossible.
Investigators further asserted that the accident’s contributing factors included the newness of the airport, a non-standard approach, high workload and stress, lack of training, and non-compliance with sterile cockpit rules. Having addressed the flight lever and subsequent loss of thrust issues, allow me to discuss the meaning behind these contributing causes.
Newness of the Airport, the Non-Standard Approach, and Workloads
As noted above, Pokhara International Airport airport opened just 14 days before the incident, on January 1, 2023. CAAN oversaw validation flights into the new airport, as well as the development of Standard Operation Procedures (SOPs) for airlines. Investigators noted, however, that CAAN had not approved SOPs for Yeti Airlines prior to authorizing validation flight. Moreover, Yeti’s validation flight did not engage in the same procedures that the incident flight later adopted. On this, investigators wrote:
During validation flight conducted by Yeti Airlines, they used runway 30 for landing and runway 12 for departure, under the supervision of CAAN inspector. Validation flight report was submitted by the inspector to CAAN. The flight was operated under day IFR principle [Instrument Flight Rules, or flying by instruments alone]. Since the airport was going to be operated only for VFR flight, the validation flight was supposed to be conducted under full VFR condition using both runways and both right hand and left hand visual circuits of RWY 12 for landings. So the recommendation for the suitability of both runways for arrival and departure without enough exercise and test seems not satisfactory. [pg. 62]
Flight 691 operated under VFR conditions and selected the downwind track for runway 12 on approach. A downwind track or leg is a common procedure flown under VFR conditions, but this was not conducted in the validation process.

This is a sample representation of the downwind track Flight 691 followed. In the image, runway 09 is where runway 12 was in the real scenario.
The report notes that YT691’s originally planned flight anticipated a landing on runway 30, not 12. Changing plans necessitated conducting this downwind track. As one pilot was instructing the other, investigators speculated that the change in approach may have been part of that instruction [pg. 64]. Adopting a last-minute flight path change undoubtedly contributed to a higher workload for the pilots, ostensibly leading to configuration changes taking place later than normal and in violation of certain standards.
SOPs, Readbacks, and Sterile Cockpit
Elevated workloads open the door for potential mistakes. The report lays out some of the workload issues during the approach that seemingly contributed to the accident.
The configuration of the aircraft for the visual approach to Pokhara may have been carried out at an altitude lower than desirable as stated in the operator’s SOPs. The operator’s SOP for Task Sharing indicates “In all situations, BOTH CMs must be aware of all important selections or switching and maintain situational awareness throughout the flight. Cross monitoring of Speed Bug / Altimeter settings / changes in frequencies / changes in aircraft configuration (Gear / Flaps) is mandatory.”
…because of the increased workload and stress, it appears as though this procedure to crosscheck and confirm switch selections was not followed. [pgs. 65 - 66]
The investigators here are saying that the various differences between the actual flight and the planned flight required enhanced attention by the flight crew, but this did not happen. All airlines adopt SOPs that assign certain tasks to the pilot flying and the pilot monitoring. This is to ensure that each stage of the flight, particularly during the landing approach, is conducted both timely and properly. A critical element of this includes robust communication between the pilots. The newness of the airport, the changes in the flight plan, and the increasingly compiling workload created a perfect storm of conditions that disintegrated the flight crew’s efficiency and effectiveness.
Investigators determined that confusion created by the increased workload basically started with the flight crew’s relative unfamiliarity with the new airport. VFR procedures for landing there had not yet been developed, so it seems the flight crew developed their own. Their plan “required tight turns during the descent and would result in the aircraft being at a lower altitude once aligned to RWY 12” [pg. 66]. This ostensibly poorly considered plan may have resulted from the fact that none of the previous demonstration flights included approaches into runway 12, only runway 30.
The report also identifies violations of sterile cockpit rules, but does not elaborate what violations specifically occurred on this flight. Generally speaking, when below 10,000 feet, flight crews can only speak about the operation of the flight. Extraneous conversation is not allowed to prevent any unnecessary distraction. Regardless of whether the pilots engaged in disallowed banter, my previous report highlighted a breakdown in communication relevant to the flight itself.
For example, a Master Chime sounded at 10:56:36. The flight crew then carried out the ‘Before Landing Checklist’ before starting the left turn onto the base leg. Nothing in the preliminary or final report indicates whether the pilots reacted to the alert, discussed it, or even noticed it. Just 14 seconds after that chime, the radio altimeter automatically called out ‘five hundred feet’ and a “click” sound was heard [pg. 13]. The torque values for both engines sat at zero by then.
The failure to annunciate a response to the chime by either crew member is one indicator of communication breakdown. Over the next few seconds, the crew discussed whether or when to continue the turn toward the airport, and the pilot monitoring called for more power. At 10:56:54, the flight data recorder (FDR) registered the flaps extending to 30 degrees. Again, no callout occurred confirming this, which is another failure of communication. ATC gave YT691 clearance to land at 10:57:07, but the flight crew did not acknowledge this.
It seems that by then the lack of power had utterly consumed their attention. This is supported by the fact that during this time and in the seconds following the power levers were shifted upward twice—though no power would be forthcoming because the engines remained in auto-feather. Control of the flight was handed over from one pilot to the other at 10:57:18, and only six seconds later the stick shaker activated.
Stick shakers provide a robust warning that an airplane faces an imminent aerodynamic stall. (Note that an aerodynamic stall means a loss of lift that keeps an aircraft airborne; it does not refer to the state of the engines). The only dialogue recorded at this point was the now-pilot-flying repeating that the engines lacked power. Shortly thereafter, the flight ended in catastrophe.
Conclusion
The final report elucidates a scenario in which the utilization of a new airport created a schism between preparation and safe operating procedures. While it identified deficiencies in both, it does not ascribe a specific reason behind either. And it is entirely possibly that there was no direct reason. Rather, the inauguration of the airport may simply have instilled confusion in the processes required to ensure that both it and the flights using it operated safely and in coordination with inbound and outbound aircraft.
The report makes numerous recommendations for procedures to follow when opening a new airport, including how airlines should handle crafting their SOPs and training protocols. Furthermore, it makes recommendations to improve CAAN’s oversight of these procedures.
It can be hard to accept that this tragedy ultimately turned on the erroneous movement of just two flight control levers. Like almost all aviation incidents, however, that single pilot error only represented the final straw in a series of mistakes that forged a tragic path to a disastrous conclusion. This is described by the so-called Swiss cheese model. Imagine stacking several pieces of Swiss cheese against each other. Single holes do not result in incidents. When the holes align, however, eventually an accident occurs. That is what happened to Yeti Airlines 691.
**My heart goes out to everyone affected by this disaster.

For a story in which the pilots intentionally deviated from safe operations, but were lucky enough to avoid tragedy, click below.

***
I am a Certified Forensic Computer Examiner, Certified Crime Analyst, Certified Fraud Examiner, and Certified Financial Crimes Investigator with a Juris Doctor and a Master’s degree in history. I spent 10 years working in the New York State Division of Criminal Justice as Senior Analyst and Investigator. Today, I teach Cybersecurity, Ethical Hacking, and Digital Forensics at Softwarica College of IT and E-Commerce in Nepal. In addition, I offer training on Financial Crime Prevention and Investigation. I am also Vice President of Digi Technology in Nepal, for which I have also created its sister company in the USA, Digi Technology America, LLC. We provide technology solutions for businesses or individuals, including cybersecurity, all across the globe. I was a firefighter before I joined law enforcement and now I currently run a non-profit that uses mobile applications and other technologies to create Early Alert Systems for natural disasters for people living in remote or poor areas.
So maybe I missed it but was that the first time they were coming to the new airport? Was the runway in a different direction than the old one or anything like that? Terrible for all those lives lost. Was everybody on that plane Nepali citizens?